
People often start wondering about aortic stenosis after something small changes: walking up a hill feels harder than it used to, you get puffed more quickly, or you notice a new heaviness in your chest that seems to come and go with effort. Sometimes it is picked up the other way around, a clinician hears a murmur during a routine visit and suggests a closer look.
It is tempting to put these shifts down to ageing, stress, or being “a bit unfit”. Those can be part of the picture, but aortic stenosis matters because it is a mechanical narrowing of the aortic valve, which can quietly increase the load on the heart for years before symptoms become obvious.1, 2, 3
Understanding what it is, how it is recognised, and what usually helps can make medical conversations clearer and reduce the chance of brushing off important warning signs.
Understanding aortic stenosis in plain terms
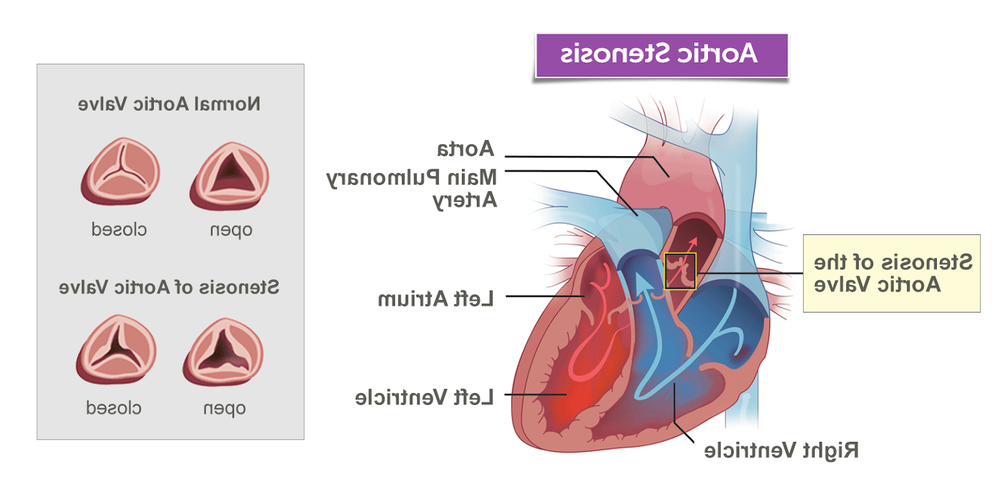
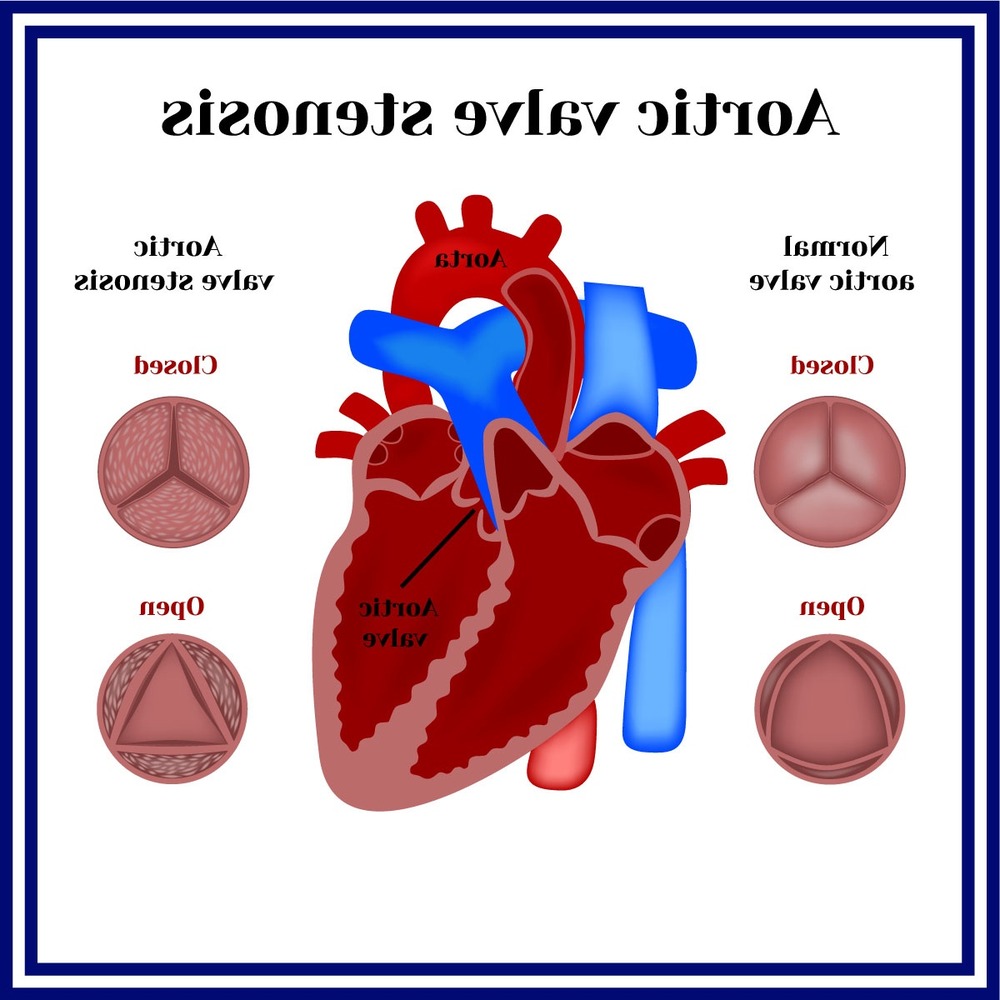
Your aortic valve sits between the left ventricle and the aorta, acting like a one-way gate that opens with each heartbeat. In aortic stenosis, the opening becomes narrower, so the heart has to push harder to move the same amount of blood forward.2, 3
Over time, that extra work can thicken the heart muscle and reduce how efficiently it fills and pumps. This is one reason symptoms often show up with activity first, when the body asks for more blood flow than the narrowed valve can comfortably deliver.2, 3
Common causes and risk factors
In adults, aortic stenosis most commonly develops as the valve stiffens and accumulates calcium with age. Another important cause is a valve that formed differently from birth, most often a bicuspid aortic valve (two leaflets instead of three), which can wear out earlier in life.2, 3
Rheumatic fever can also damage heart valves and contribute to stenosis, although it is less common in places where streptococcal infections are promptly treated.2
Factors that tend to travel alongside aortic stenosis, and are still worth managing carefully, include high blood pressure, high cholesterol, diabetes, smoking, and chronic kidney disease. They do not always “cause” the valve narrowing directly, but they can influence overall cardiovascular risk and how well someone copes with the condition.2, 5
Symptoms people notice, and why they can be missed
Aortic stenosis can be present for a long time without clear symptoms. When symptoms do appear, they often include:
- Breathlessness with activity
- Chest pain, tightness, or pressure, especially on exertion
- Dizziness or fainting, particularly with exertion
- Unusual fatigue, or a noticeable drop in exercise tolerance
- Palpitations (an uncomfortable awareness of heartbeat)
- Swelling in the ankles or feet if heart failure develops
Several of these can overlap with asthma, lung conditions, anaemia, deconditioning, or “just getting older”. That overlap is part of what delays diagnosis for some people, especially if changes are gradual.2, 3, 4
How aortic stenosis is diagnosed
Many diagnoses begin with a clinical exam. A clinician may hear a murmur, ask more detailed questions about exertional symptoms, and look for signs of fluid retention or reduced circulation.
The key test is usually an echocardiogram (heart ultrasound). It shows the valve anatomy, how tightly it opens, and how the narrowing is affecting pressures and heart function.2, 6
Other tests that may be used
Depending on symptoms and the clinical question, clinicians may add other investigations, such as an ECG, chest X-ray, blood tests, exercise testing, or CT imaging to assess valve calcification and plan procedures. These do not replace echocardiography, but they can help clarify severity and guide next steps.6, 7
Why early detection matters
There is a particular challenge with aortic stenosis: the valve does not typically “open up again” with tablets or lifestyle changes alone. People can feel well for years, then deteriorate more quickly once the narrowing becomes severe and the heart is under strain.2, 7
Early detection is not about rushing everyone into a procedure. It is about matching follow-up to risk, understanding what symptoms to watch for, and planning ahead if the stenosis becomes severe. Many people do best when decisions are made before a crisis point, not after.2, 4, 7
If symptoms are sudden, severe, or concerning, particularly chest pain, fainting, or significant breathlessness, urgent medical assessment is appropriate.3
Treatment options, from monitoring to valve replacement
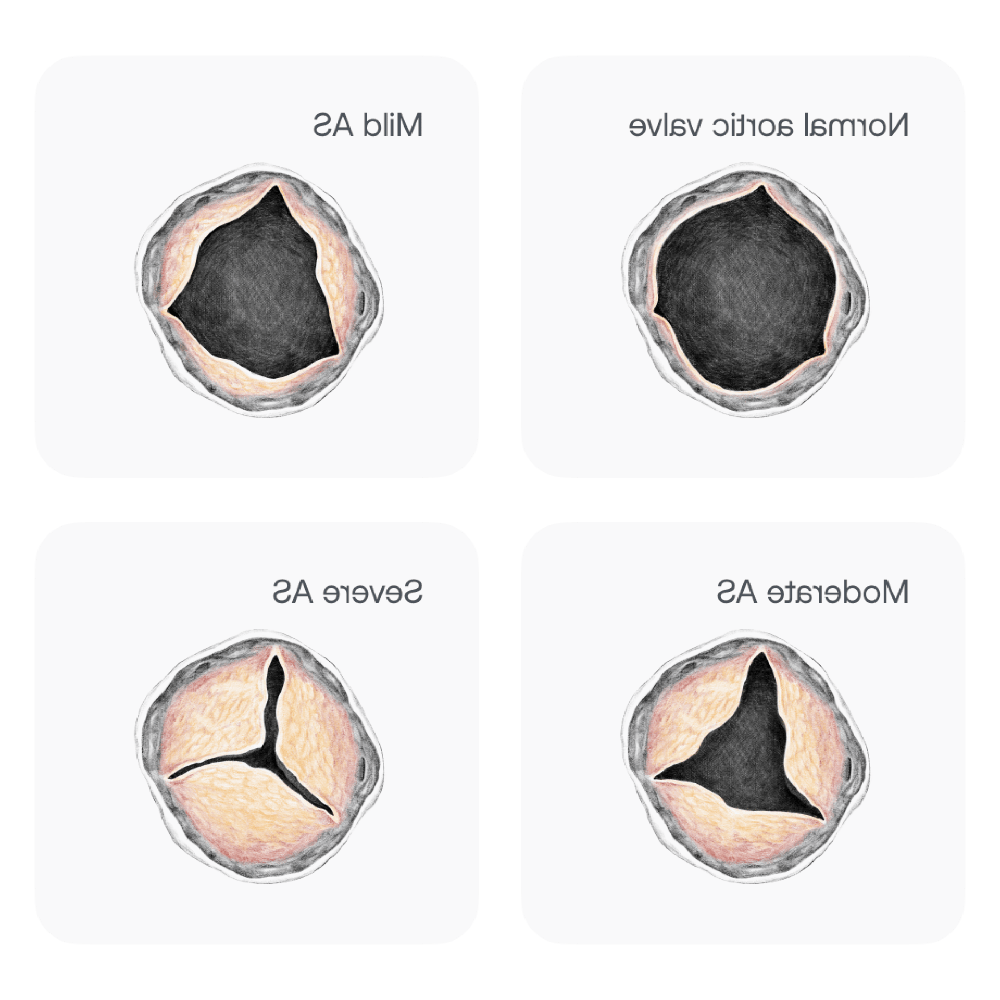
Treatment depends on severity, symptoms, and overall health. Mild or moderate aortic stenosis is often managed with monitoring and risk-factor care. Severe aortic stenosis, particularly when symptoms are present, is commonly treated with aortic valve replacement.2, 4, 7
Medicines: helpful, but not a “fix” for the valve
Medicines may be used to manage blood pressure, fluid overload, cholesterol, heart rhythm problems, or other co-existing heart disease. They can improve comfort and reduce risk, but they do not reliably reverse the narrowing itself.2, 7
Valve replacement procedures
When replacement is recommended, the main approaches are:
- Surgical aortic valve replacement (SAVR), an open procedure where the valve is replaced.
- Transcatheter aortic valve implantation or replacement (TAVI or TAVR), a less invasive approach where a new valve is delivered by catheter, often via an artery in the groin.
Which option is best depends on age, anatomy, surgical risk, other medical conditions, and personal priorities, including recovery time and the likely durability of different valve types.7, 8
Living with aortic stenosis day to day
For many people, the practical work is not dramatic. It looks like paying attention to patterns, keeping appointments, and making a few steady choices that reduce strain on the heart.
If you have been diagnosed, it can help to keep a brief note of symptoms and triggers, for example breathlessness on stairs, chest discomfort with exertion, near-fainting, or a noticeable fall in walking distance. Subtle changes are often the most useful ones to bring to your clinician.4, 6
Helpful habits and risk reduction
Even though lifestyle changes do not “un-narrow” the valve, they can support heart function and lower overall cardiovascular risk. The basics still matter:
- Stay physically active within your clinician’s advice, aim for regular, moderate movement rather than sudden, intense bursts.
- Choose a heart-healthy eating pattern, and manage weight in a realistic, sustainable way.
- Do not smoke, and ask for support to quit if needed.
- Keep blood pressure, diabetes, and cholesterol well controlled.
- Prioritise dental care, and seek prompt treatment for infections, since valve disease can increase susceptibility to infective endocarditis in some circumstances.4, 9
Follow-up intervals vary. Some people need echocardiograms every few years, others more often. The aim is to time monitoring so changes are caught early, especially if stenosis is progressing or symptoms are emerging.2, 6
Where research is heading
Research in aortic stenosis continues to focus on better imaging, improving procedural safety, refining who benefits most from early intervention, and developing longer-lasting valve technologies. There is also ongoing work on understanding the biology of valve calcification, although there is not yet a medicine that reliably stops or reverses the narrowing in the way replacement can for severe disease.7, 8
For someone living with aortic stenosis, the most meaningful “innovation” often looks like clearer timing: knowing when watchful waiting is sensible, and when it is time to discuss replacement before daily life becomes smaller and more restricted.2, 4, 7
Final thoughts
Aortic stenosis is sometimes first noticed as a change in stamina, sometimes as a murmur, and sometimes only after a period of slowly adapting to symptoms. The condition is common, treatable, and often manageable for a long time with the right follow-up. When replacement is needed, it is usually because the valve has become too tight for the heart to compensate safely.
If you are noticing breathlessness, chest discomfort with exertion, dizziness, or a drop in your usual capacity, it is reasonable to raise it with a clinician and ask whether a murmur or an echocardiogram assessment is appropriate.2, 3, 6
References
- American Heart Association: Aortic Stenosis Overview
- Mayo Clinic: Aortic valve stenosis (symptoms and causes)
- Cleveland Clinic: Aortic stenosis (symptoms and treatment)
- American Heart Association: Managing aortic stenosis symptoms
- Australian Institute of Health and Welfare: Cardiovascular disease risk factors
- healthdirect Australia: Aortic stenosis (symptoms, causes, diagnosis and treatment)
- European Society of Cardiology: Valvular heart disease guidelines
- CardioSmart (American College of Cardiology): Aortic stenosis treatment and management
- Heart Foundation (Australia): Infective endocarditis